Gallbladder Cancer in North India: Why It’s Often Diagnosed Late
Gallbladder cancer is disproportionately common in North India and tragically diagnosed late. Understand the reasons, risk factors, and early warning signs.
Get a free second opinion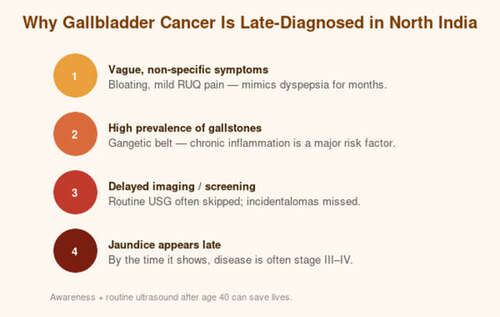
Gallbladder cancer is disproportionately common in North India and tragically diagnosed late. Understand the reasons, risk factors, and early warning signs.
Gallbladder cancer is a disease with an uncomfortable geographic signature. While it is rare in most of the world, it is one of the most common gastrointestinal cancers in the Gangetic plains of North India — particularly Bihar, Uttar Pradesh, West Bengal, and parts of Jharkhand. The incidence in women in some districts of North India is among the highest ever recorded anywhere in the world. And yet, despite this grim distinction, gallbladder cancer remains one of the most commonly missed diagnoses in Indian medicine, because its early symptoms are almost indistinguishable from everyday dyspepsia. By the time most patients are diagnosed, the disease has already spread. This article explains why — and what can be done to change it.
The North Indian epidemic
Epidemiological studies consistently show that the age-adjusted incidence of gallbladder cancer in women in the Gangetic belt is between 10 and 22 per 100,000 — ten to twenty times higher than the national Indian average, and over fifty times higher than in most of the Western world. The reasons are still being investigated, but three factors are widely accepted: an unusually high prevalence of gallstones, chronic exposure to heavy metals in drinking water (particularly arsenic), and a genetic susceptibility that runs in certain communities.
The result is a disease that families often know about — someone’s aunt, someone’s neighbour — but do not recognize in themselves until it is far too late.
Why it is diagnosed so late
Early gallbladder cancer produces no specific symptoms. Patients may experience vague upper-abdominal discomfort, mild bloating after fatty meals, or a sense of fullness — all symptoms that are routinely attributed to ‘gas’ or ‘acidity.’ When pain does become prominent, it often overlaps with the symptoms of gallstones, which are extremely common in the same population. A patient may be treated for years for stone-related pain before anyone suspects cancer.
Jaundice, the symptom most people associate with gallbladder disease, is typically a late sign. By the time the skin and eyes turn yellow, the tumour has usually blocked the bile duct — which means the cancer has already extended beyond the gallbladder wall. Weight loss, loss of appetite, and a palpable mass in the upper abdomen are also late findings.
Compounding the delay, routine abdominal ultrasound — the single most effective screening tool — is not performed regularly in most primary care settings, and incidental gallbladder wall thickening is often dismissed as chronic cholecystitis.
Known risk factors
The classical risk factors for gallbladder cancer include: gallstones (particularly larger stones >3 cm, present for over 10 years), gallbladder polyps larger than 1 cm, porcelain gallbladder, chronic typhoid carriage, obesity, and female sex. In North India, additional regional factors include arsenic-contaminated groundwater, mustard oil consumption patterns, and specific genetic polymorphisms in xenobiotic-metabolizing enzymes.
Perhaps the most important risk factor to remember is also the most common: any gallstone, present for many years, particularly in a woman over 50 in the Gangetic belt, is a small but real cancer risk.
What early detection looks like
Early detection depends on two things: recognizing who is at risk, and not dismissing vague upper-abdominal symptoms. Any woman over 40 in North India with persistent right-upper-quadrant discomfort, with or without known gallstones, deserves an ultrasound. If the ultrasound shows gallbladder wall thickening, a polyp larger than 10 mm, or any suspicious finding, the next step is a contrast-enhanced CT scan and a surgical opinion.
In some selected high-risk patients — those with large gallstones, porcelain gallbladder, polyps larger than 1 cm, or a strong family history — prophylactic cholecystectomy (removal of the gallbladder) should be seriously considered, even in the absence of cancer. The operation is routine and low-risk, and it eliminates the future cancer risk entirely.
Treatment and realistic outcomes
Treatment depends entirely on stage. Very early disease (incidentally discovered after routine cholecystectomy for stones) can often be cured by a second surgery that removes additional liver tissue and lymph nodes around the gallbladder fossa — an operation called extended cholecystectomy. Locally advanced disease may require more extensive liver resection and bile duct reconstruction. Advanced disease is treated with chemotherapy, with targeted and immunotherapy options emerging.
Five-year survival for Stage I gallbladder cancer after surgery is 60–80%. For Stage III, it drops to 20–30%, and for Stage IV, under 5%. The single most important determinant of survival is stage at diagnosis — which means that awareness and early imaging are, quite literally, life-saving in North India. If you live in the Gangetic belt, please do not ignore persistent upper-abdominal symptoms.
Frequently Asked Questions
If I have gallstones, should I get my gallbladder removed?
Not all gallstones need surgery. But in North India — particularly for women over 40 with large stones, a long history of stones, or symptoms — prophylactic cholecystectomy is often recommended because of the regional cancer risk. Discuss with a GI surgeon.
Is gallbladder cancer curable?
Yes, if caught at Stage I or II and treated with appropriate surgery at an experienced center. Early-stage 5-year survival approaches 70–80%. The challenge is catching it early.
What is an incidental gallbladder cancer?
It is gallbladder cancer found unexpectedly in a gallbladder removed for stones. If this happens to you, a second opinion from an HPB surgeon is essential — a second, more extensive operation is often needed to complete the cancer treatment.
Can imaging reliably detect early gallbladder cancer?
A high-quality abdominal ultrasound detects most suspicious lesions. A contrast-enhanced CT or MRI provides staging. Early cancers can be subtle, so experienced radiology matters.
Consult Dr. Abhishek Aggarwal
Associate Director — GI, HPB & Cancer Surgery

Meet Dr. Abhishek Aggarwal
Dr. Abhishek Aggarwal is a highly skilled GI & HPB surgeon with over 10 years of experience in managing complex gastrointestinal and hepato-pancreato-biliary diseases, with a special focus on oncological surgery. He currently serves as Associate Director – GI Oncosurgery at BLK-Max Super Speciality Hospital, where he is actively involved in delivering advanced surgical care for GI and HPB malignancies.
He has trained and worked in reputed high-volume centres, gaining extensive expertise in complex oncological procedures and multidisciplinary cancer care. His clinical practice is firmly grounded in scientific, evidence-based medicine, ensuring that patients receive treatment aligned with the latest global standards and research.
OPD Timing: 09:00 AM – 05:00 PM
Contact Dr. Abhishek →