HIPEC Surgery: A New Hope for Peritoneal Cancer Patients
HIPEC (hyperthermic intraperitoneal chemotherapy) can extend survival for selected peritoneal cancer patients. Learn how it works, who benefits, and what to expect.
Get a free second opinion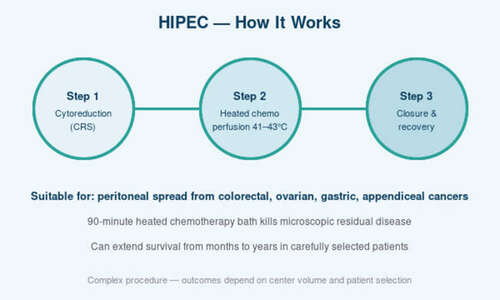
HIPEC (hyperthermic intraperitoneal chemotherapy) can extend survival for selected peritoneal cancer patients. Learn how it works, who benefits, and what to expect.
For decades, cancer that had spread to the lining of the abdominal cavity — the peritoneum — was considered essentially untreatable. Patients were offered palliative chemotherapy and told to prepare for the worst. Over the last 20 years, a combination of aggressive cytoreductive surgery and a specialized technique called HIPEC — hyperthermic intraperitoneal chemotherapy — has rewritten the outlook for carefully selected patients with certain peritoneal cancers. It is not a cure for everyone, and it is not suitable for every patient. But for the right person, HIPEC can convert a disease that was once a death sentence into one that offers years of high-quality life. This article explains what HIPEC actually is, who genuinely benefits from it, and what to expect from the procedure.
The problem HIPEC is designed to solve
Certain cancers — particularly those of the appendix, ovary, colon, and stomach — have a tendency to spread across the surface of the peritoneum rather than through the bloodstream. This pattern of spread, called peritoneal carcinomatosis, is difficult to treat with traditional chemotherapy because intravenous drugs do not penetrate the abdominal lining effectively.
HIPEC solves this problem directly. After the surgeon meticulously removes every visible piece of cancer from the abdomen (the ‘cytoreduction’ part), heated chemotherapy is pumped directly into the abdominal cavity for 60–90 minutes. The heat makes the chemotherapy much more effective, and because the drug is delivered inside the abdomen at a very high local concentration, it can kill microscopic disease that intravenous chemotherapy would miss.
Who benefits — patient selection is everything
HIPEC is a major operation and is not suitable for every patient with peritoneal spread. The ideal candidates are patients with: pseudomyxoma peritonei (a rare appendiceal cancer), peritoneal spread from colon or rectal cancer with a limited disease burden, peritoneal mesothelioma, some ovarian cancers after chemotherapy, and select gastric cancers with minimal peritoneal disease.
The single most important factor is whether a ‘complete cytoreduction’ — removing every visible piece of tumour — is technically achievable. This depends on the volume and location of disease, often measured using a score called the Peritoneal Cancer Index (PCI). Patients with low PCI scores and disease confined to accessible areas are the best candidates. Those with extensive, bulky disease in multiple quadrants are often not.
What the procedure actually involves
A full HIPEC procedure is long — typically 8 to 14 hours. The first and most important phase is cytoreductive surgery. The surgeon systematically explores the entire abdomen, removing every cancer deposit visible to the eye. This may require removal of parts of the peritoneum, portions of the bowel, the spleen, the gallbladder, and sometimes the uterus and ovaries. It is one of the most demanding operations in all of cancer surgery and should only be performed by a team specifically trained in the technique.
Once cytoreduction is complete, the HIPEC phase begins. A chemotherapy solution (commonly mitomycin C, oxaliplatin, or cisplatin, depending on the cancer type) is warmed to 41–43°C and circulated through the abdomen for 60–90 minutes via catheters placed during surgery. The surgeon gently rocks the patient during the perfusion to ensure even drug distribution. After the perfusion, the abdomen is flushed, drains are placed, and the abdomen is closed.
Recovery and the realistic outlook
HIPEC is a demanding recovery. Patients typically spend 2–4 days in the ICU and 10–14 days in hospital. Fatigue, loss of appetite, and gradual weight loss in the first month are normal. Return to pre-operative energy levels usually takes 2–3 months. The complication rate — 25–40% in most published series — is real and reflects the complexity of the operation. At experienced centers, the 90-day mortality is under 3%.
The oncological benefit, for the right patient, is profound. Patients with pseudomyxoma peritonei treated with complete cytoreduction and HIPEC have 5-year survival rates over 70%. For peritoneal spread from colon cancer, 5-year survival after successful HIPEC is 30–40%, compared to under 5% with chemotherapy alone. These are not incremental improvements — they are life-changing differences for patients who were previously told there was nothing more to be done.
Choosing where to have HIPEC
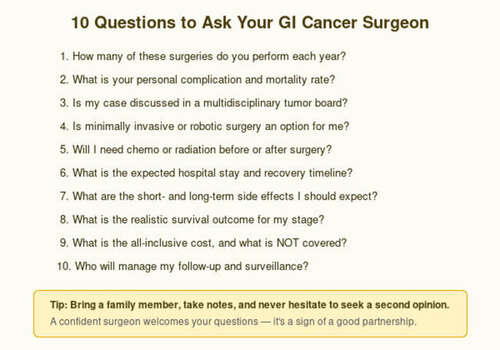
HIPEC is the paradigm case of an operation where the choice of center matters enormously. The learning curve is steep, the intra-operative decisions are complex, and complication management requires experienced critical care. Look for a center that performs at least 20 HIPEC procedures a year, has a dedicated peritoneal malignancy team, and can show you their published outcomes. Ask specifically about the Peritoneal Cancer Index of patients they have treated, their complete cytoreduction rate, and their 30- and 90-day mortality.
If you or a loved one has been told that peritoneal cancer spread leaves ‘no options,’ please seek a second opinion from a peritoneal malignancy center before accepting that conclusion. You may not be a candidate — but you may be — and the difference is worth finding out.
Frequently Asked Questions
Is HIPEC a cure for peritoneal cancer?
For pseudomyxoma peritonei and some other select cancers, HIPEC can achieve long-term cure in a meaningful percentage of patients. For others, it can extend survival from months to years. Patient selection is the critical factor.
How long does HIPEC surgery take?
The full procedure typically lasts 8–14 hours, depending on the extent of disease and the cytoreduction required. It should only be performed at experienced centers.
What are the main risks of HIPEC?
The major risks include infection, anastomotic leak, bleeding, kidney injury from chemotherapy, and prolonged recovery. Complication rates of 25–40% are typical, but the vast majority are manageable at experienced centers.
How is HIPEC different from regular chemotherapy?
Regular chemotherapy is given intravenously and treats the whole body. HIPEC delivers heated chemotherapy directly into the abdominal cavity after surgery, allowing much higher local drug concentrations without the systemic side effects.
Consult Dr. Abhishek Aggarwal
Associate Director — GI, HPB & Cancer Surgery

Meet Dr. Abhishek Aggarwal
Dr. Abhishek Aggarwal is a highly skilled GI & HPB surgeon with over 10 years of experience in managing complex gastrointestinal and hepato-pancreato-biliary diseases, with a special focus on oncological surgery. He currently serves as Associate Director – GI Oncosurgery at BLK-Max Super Speciality Hospital, where he is actively involved in delivering advanced surgical care for GI and HPB malignancies.
He has trained and worked in reputed high-volume centres, gaining extensive expertise in complex oncological procedures and multidisciplinary cancer care. His clinical practice is firmly grounded in scientific, evidence-based medicine, ensuring that patients receive treatment aligned with the latest global standards and research.
OPD Timing: 09:00 AM – 05:00 PM
Contact Dr. Abhishek →