Whipple Surgery Explained: Procedure, Recovery & Success Rate
A complete patient’s guide to Whipple surgery (pancreaticoduodenectomy) — what happens, how long recovery takes, success rates, and questions to ask your surgeon.
Get a free second opinion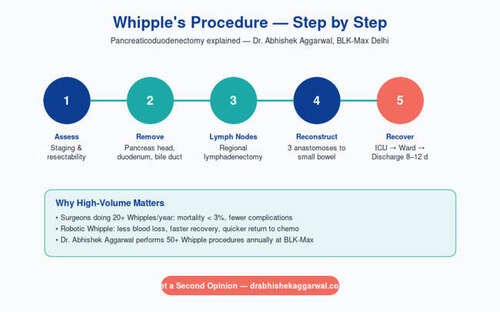
A complete patient’s guide to Whipple surgery (pancreaticoduodenectomy) — what happens, how long recovery takes, success rates, and questions to ask your surgeon.
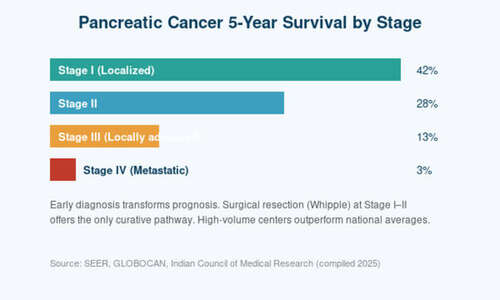
Few operations in modern medicine are as technically complex — or as life-saving — as the Whipple procedure. Formally known as pancreaticoduodenectomy, it is the only potentially curative treatment for cancers of the pancreatic head, ampulla, distal bile duct, and duodenum. Patients who hear they need a Whipple are often overwhelmed by its reputation as a ‘big surgery.’ That reputation is not undeserved — it is one of the largest operations performed on the human abdomen. But it is also, in experienced hands, one of the most successful: with modern techniques, mortality at high-volume centers is now under 2%, and long-term cure is a realistic outcome for many patients. This guide demystifies the Whipple — what actually happens in the operating room, what recovery is really like, and what questions you should ask before consenting to surgery.
What a Whipple actually removes
The Whipple procedure removes a surprising amount of anatomy, because the pancreatic head sits at a crossroads where several organs share a blood supply. In a standard Whipple, the surgeon removes: the head of the pancreas, the entire duodenum (first part of the small intestine), the gallbladder, the distal bile duct, and a portion of the stomach (in the classical Whipple) or just the pylorus (in the pylorus-preserving variant). Nearby lymph nodes are also removed for staging.
Once this block of tissue is out, the reconstruction begins. Three new connections are created: the remaining pancreas is joined to a loop of small intestine (pancreaticojejunostomy), the bile duct is joined to the same loop (hepaticojejunostomy), and the stomach is joined further down (gastrojejunostomy). These three anastomoses are the heart of the operation — and the place where complications, when they occur, usually arise.
How long the surgery takes — and why it varies
A straightforward Whipple takes between 4 and 7 hours. Complex cases — particularly those involving reconstruction of the portal vein or superior mesenteric vein — can take 8 to 10 hours. The time is driven not by rushing but by the meticulous dissection required around major blood vessels. A surgeon who finishes a Whipple in three hours is not a better surgeon; they are a faster one, and speed is not a virtue in this operation.
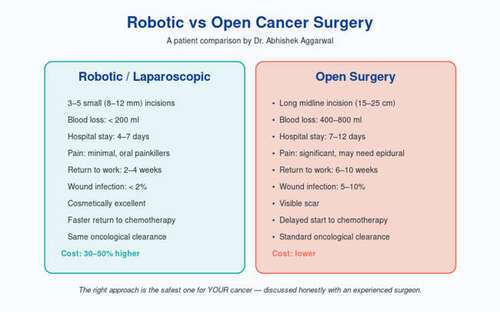
Modern centers are increasingly offering laparoscopic and robotic Whipples. In experienced hands, these can shorten recovery and reduce blood loss. However, they are technically even more demanding than the open approach, and should only be performed at high-volume centers with proven minimally invasive HPB programs.
What to expect in the hospital
Patients typically spend the first 24–48 hours in the intensive care unit for close monitoring of heart, lungs, and fluid balance. Pain is managed with epidural anaesthesia or intravenous medications. On day 2 or 3, most patients begin sitting out of bed. By day 3 or 4, clear liquids are usually started, progressing gradually to soft foods.
Drains are placed at the time of surgery and are removed one by one as output decreases. The total hospital stay at an experienced Indian center is typically 7–10 days. Patients go home on oral medications, sometimes with a temporary feeding tube if nutrition is a concern.
Recovery at home — a realistic timeline
Week 1–2 at home: low energy, small frequent meals, short walks. Expect to nap during the day. Week 3–4: appetite begins to recover, walks get longer. Week 5–6: most patients can return to light office work. Full recovery — return to pre-surgery energy and strength — typically takes 2 to 3 months.
During recovery, certain symptoms are normal: mild abdominal bloating, some loose stools (especially after fatty meals), and weight loss of 3–5 kg. Pancreatic enzyme supplements taken with meals help digestion and usually prevent severe weight loss. Some patients develop diabetes after surgery because a portion of the insulin-producing pancreas has been removed — this is managed with oral medications or insulin as needed.
Success rates, complications, and the volume effect
At high-volume centers (>25 Whipples per year), peri-operative mortality is now 1–3%, and serious complications occur in about 30–35% of patients — most of them manageable. At low-volume centers, mortality can be 5–6 times higher. This single fact — the volume–outcome relationship — is the most important thing a prospective Whipple patient should understand.
The most serious complication is a pancreatic fistula — leakage from the pancreaticojejunostomy. Most are minor and heal on their own; a small minority require drainage or reoperation. Other complications include delayed gastric emptying, infection, bleeding, and diabetes. Long-term, most patients return to a full, normal life within 3 months.
Frequently Asked Questions
Is a Whipple always for cancer?
No. About 85% of Whipples are done for malignant disease (pancreatic, ampullary, bile duct, or duodenal cancer), but some are performed for benign conditions such as chronic pancreatitis, neuroendocrine tumours, and certain cysts.
How should I choose a Whipple surgeon?
Ask two questions: how many Whipples does your team perform every year, and what is your personal complication and mortality rate? A confident surgeon will answer both openly. Aim for a center with >25 cases per year.
Will I live a normal life after a Whipple?
Most patients return to normal life within 3 months. Long-term adjustments include taking pancreatic enzyme supplements with meals and, in some cases, managing new-onset diabetes.
Can a Whipple be done laparoscopically or robotically?
Yes, in experienced centers. Robotic Whipple offers faster recovery but is technically more demanding. Ask your surgeon about their specific minimally invasive experience.
Consult Dr. Abhishek Aggarwal
Associate Director, BLK-Max Delhi — GI, HPB & Cancer Surgery
Pancreatic Cancer Survival Rate in India — What the Numbers Really Mean
Robotic vs Open Cancer Surgery: Which Is Better and When?

Meet Dr. Abhishek Aggarwal
Dr. Abhishek Aggarwal is a highly skilled GI & HPB surgeon with over 10 years of experience in managing complex gastrointestinal and hepato-pancreato-biliary diseases, with a special focus on oncological surgery. He currently serves as Associate Director – GI Oncosurgery at BLK-Max Super Speciality Hospital, where he is actively involved in delivering advanced surgical care for GI and HPB malignancies.
He has trained and worked in reputed high-volume centres, gaining extensive expertise in complex oncological procedures and multidisciplinary cancer care. His clinical practice is firmly grounded in scientific, evidence-based medicine, ensuring that patients receive treatment aligned with the latest global standards and research.
OPD Timing: 09:00 AM – 05:00 PM
Contact Dr. Abhishek →