Pancreatic Cancer Survival Rate in India — What the Numbers Really Mean
Pancreatic cancer survival depends on stage, surgery, and specialist center volume. Understand the real numbers for India in 2026 and what they mean for you.
Get a free second opinion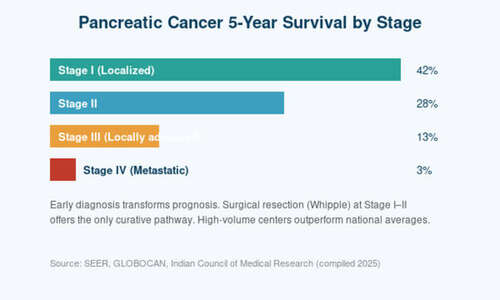
Pancreatic cancer survival depends on stage, surgery, and specialist center volume. Understand the real numbers for India in 2026 and what they mean for you.
When a patient hears the words “pancreatic cancer,” the first question is almost always the same: “How long do I have?” It is a natural, human question — but also one of the most misunderstood in oncology. The headline statistic most patients find on the internet — that pancreatic cancer has a 5-year survival rate of under 10% — is technically true, but deeply misleading. That number bundles together every stage, every patient, every hospital, and every year going back decades. Your situation is not the average. The real survival rate for pancreatic cancer depends on three things that actually matter: what stage the cancer is at, whether you are a candidate for surgery, and where you are being treated. This article walks you through what the numbers really mean in India in 2026 — and where there is room for genuine hope.
The headline number, and why it is misleading
The widely quoted 5-year survival rate for pancreatic cancer in India is approximately 8–10%. This figure is often presented as if it were a prognosis, but it is not. It is an average across every patient ever diagnosed, including those discovered at Stage IV, those who never received treatment, those treated decades ago before modern chemotherapy, and those treated at centers with little experience in pancreatic surgery.
When you break the number down by stage and treatment center, a very different picture emerges. Patients diagnosed at Stage I who undergo a successful Whipple procedure at a high-volume center have 5-year survival rates approaching 40–45%. Some subgroups do even better. The honest answer to ‘how long do I have?’ is always: it depends — and many of the factors are within your control.
Survival by stage — the numbers that matter
Stage I (localized, tumour <2 cm, no node involvement): 5-year survival 40–45% with surgery. These patients have the best chance of long-term cure. Unfortunately, only 10–15% of Indian patients are diagnosed at this stage.
Stage II (tumour extends beyond pancreas but still resectable): 5-year survival 25–30% with surgery plus adjuvant chemotherapy. This is the most common ‘operable’ group.
Stage III (locally advanced, involves major blood vessels): 5-year survival 10–15%. Modern neoadjuvant chemotherapy — giving chemo first to shrink the tumour — has recently allowed many Stage III patients to become surgical candidates.
Stage IV (distant metastasis): 5-year survival under 5%. Treatment focuses on extending life and maintaining quality of life, not cure. However, median survival has improved meaningfully with modern FOLFIRINOX and gemcitabine-nab paclitaxel regimens.
Why the center where you are treated makes a huge difference
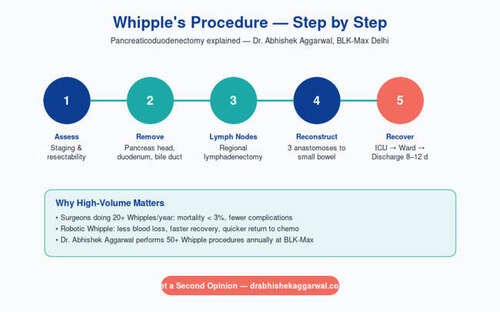
Pancreatic surgery is one of the most technically demanding operations in all of medicine. The pancreas sits surrounded by critical blood vessels; one misstep can be catastrophic. Decades of international data now confirm a simple truth: hospitals and surgeons who perform a high volume of pancreatic operations have dramatically better outcomes. A 2019 meta-analysis showed that mortality after a Whipple operation can be as low as 1–2% at high-volume centers and as high as 10–15% at low-volume ones.
This is the single most important decision a pancreatic cancer patient will make. If you are advised that you need a Whipple, seek treatment at a center that performs at least 25 Whipples a year, with a dedicated HPB (hepatopancreatobiliary) team. The difference is not marginal — it is often the difference between cure and tragedy.
What has changed in the last five years
The last half-decade has seen real, measurable progress in pancreatic cancer care in India. Three developments stand out. First, neoadjuvant therapy — chemo before surgery — is now standard for borderline-resectable and locally advanced disease, and has converted many previously inoperable cases into curative surgeries. Second, minimally invasive and robotic Whipple procedures are being offered in select Indian centers, with shorter recovery and less blood loss in experienced hands. Third, molecular testing for BRCA mutations and other targets has opened the door to personalized therapy in a disease where it was previously unheard of.
What this means for you and your family
If you or a loved one has just been diagnosed with pancreatic cancer, here is the practical path forward. Step one: get the full staging done. You need a triple-phase CT scan of the pancreas, not a regular abdominal scan, plus tumour markers (CA 19-9) and an endoscopic ultrasound with biopsy. Step two: get a second opinion at a high-volume HPB center before starting any treatment. The treatment plan from a dedicated pancreatic team is often meaningfully different from the first recommendation. Step three: ask explicitly whether you are a candidate for surgery, for neoadjuvant therapy, or for a clinical trial.
Pancreatic cancer is a serious diagnosis, but the era of universal hopelessness is over. Early-stage patients can be cured. Locally advanced patients are increasingly making it to surgery. And even Stage IV patients are living longer, better lives than they were a decade ago. The numbers only tell half the story — your choices fill in the rest.
Frequently Asked Questions
What is the survival rate after a successful Whipple surgery?
For Stage I–II disease treated at a high-volume center, 5-year survival after Whipple is typically 30–45%. Younger patients, smaller tumours, and clear surgical margins are associated with the best outcomes.
Can pancreatic cancer be cured?
Yes, but only when caught early and treated with complete surgical resection followed by adjuvant chemotherapy. Cure is possible for Stage I and some Stage II patients.
Is pancreatic cancer hereditary?
About 10% of pancreatic cancers have a genetic component. BRCA1, BRCA2, and Lynch syndrome mutations increase risk. If two or more close relatives have had pancreatic cancer, ask about genetic counselling.
Should I get a second opinion?
Yes, always — particularly from a high-volume HPB surgical team. The treatment plan can differ meaningfully, and your long-term outcome depends heavily on the team that treats you.
Consult Dr. Abhishek Aggarwal
Associate Director — GI, HPB & Cancer Surgery

Meet Dr. Abhishek Aggarwal
Dr. Abhishek Aggarwal is a highly skilled GI & HPB surgeon with over 10 years of experience in managing complex gastrointestinal and hepato-pancreato-biliary diseases, with a special focus on oncological surgery. He currently serves as Associate Director – GI Oncosurgery at BLK-Max Super Speciality Hospital, where he is actively involved in delivering advanced surgical care for GI and HPB malignancies.
He has trained and worked in reputed high-volume centres, gaining extensive expertise in complex oncological procedures and multidisciplinary cancer care. His clinical practice is firmly grounded in scientific, evidence-based medicine, ensuring that patients receive treatment aligned with the latest global standards and research.
OPD Timing: 09:00 AM – 05:00 PM
Contact Dr. Abhishek →